
How to Cite
Copyright notice

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Copyright (c) 2024 Nor Hidayah Zainool Abidin, Norhafidzah Ghazali, Fazilawati Zakaria, Nor Izatul Azma Azhar




Keywords
Abstract
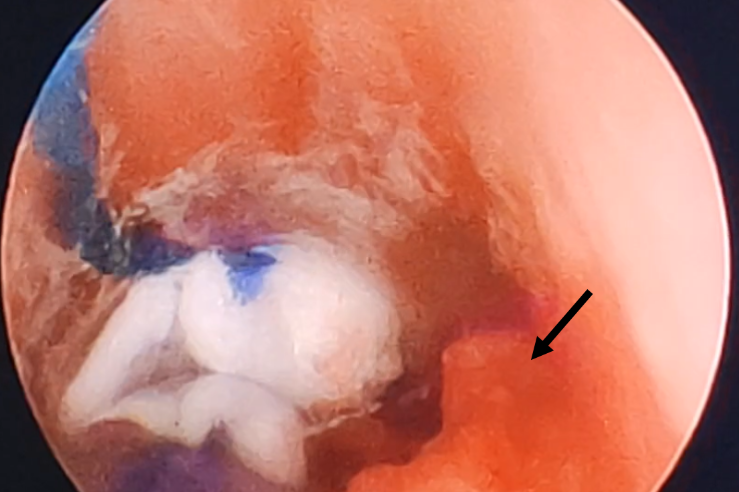
Tracheal stenosis secondary to tumour presents potential airway complications such as bleeding, airway oedema, laryngospasm and bronchospasm secondary to airway irritation, and difficulty advancing the endotracheal tube through the slit-like diameter of the trachea lumen. We present a case with double pathology of goitre and intraluminal tracheal tumour for thyroidectomy and tumour biopsy. A multidisciplinary discussion was held preoperatively between the otorhinolaryngology surgeons, radiologist, and anaesthesiologists to define resectability and perioperative management. The awake fibreoptic intubation oral approach using a microlaryngoscopy tube size 5 with target-controlled infusion of remifentanil sedation was successful. The airway was anaesthetised with a sphenopalatine ganglion block, palatopharyngeal arch nerve block, nebulisation lignocaine, and spray-as-you-go lignocaine to obtund the pharyngeal and laryngeal reflexes. Post thyroidectomy,
direct rigid laryngoscopy was performed for tumour biopsy. The patient was later admitted to the intensive care unit for postoperative ventilation and monitoring. We learned that there is no single universal airway technique for airway management as it should be tailored based on the individual patient’s airway pathology and comorbidities after careful perioperative discussion and airway planning.
References
Ghaloo SK, Afzal SS, Abbas SA, Ansari S, De M, Iftikhar H. Tracheomalacia in patients undergoing thyroid surgery—What is the true estimate: A systematic review and meta-analysis. World Journal of Otorhinolaryngology - Head and Neck Surgery. 2024 May 15:1-13. https://doi.org/https://doi.org/10.1002/wjo2.182
Malpas G. Clinical Airway Management: An Illustrated Case-Based Approach. Can J Anesth. 2018 Feb;65:229-30. https://doi.org/10.1007/s12630-017-0985-y
Satoh M, Hirabayashi Y, Seo N. Spontaneous breathing combined with high frequency ventilation during bronchoscopic resection of a large tracheal tumour. Br J Anaesth. 2002 Oct;89(4):641-3. https://doi.org/10.1093/bja/aef223
Ran G, Ning M, Zhang X. Awake fiberoptic intubation in a patient with a large thyroid tumor invading the trachea: a case report. Am J Transl Res. 2022 Apr 15;14(4):2497-500.
Marwaha A, Kumar A, Sharma S, Sood J. Anaesthesia for tracheal resection and anastomosis. J Anaesthesiol Clin Pharmacol. 2022 Jan-Mar;38(1):48-57. https://doi.org/10.4103/joacp.JOACP_611_20
Koul A, Sood J. Leiomyoma of trachea: An anaesthetic challenge. Indian J Anaesth. 2013 Jul-Aug;57(4):412-4. https://doi.org/10.4103/0019-5049.118543
Sinnatamby CS, Last RJ. Last’s anatomy: regional and applied. 2011.
Uludağ M, Tanal M, İşgör A. A Review of Methods for the Preservation of Laryngeal Nerves During Thyroidectomy. Sisli Etfal Hastan Tip Bul. 2018 Jun 18;52(2):79-91. https://doi.org/10.14744/semb.2018.37928
Umstot R, Samanta D, Umstot E, Area SA, Richmond BK, Jarrouj A. Ten-Year Review of Tracheostomy Techniques and Related Complications. Am Surg. 2024 Feb;90(2):225-30. https://doi.org/10.1177/00031348231198115
Hofmeyr RH, Llewellyn R, Fagan JJ. Multidisciplinary difficult airway challenges: Perioperative management of glottic and supraglottic tumors. Operative Techniques in Otolaryngology-Head and Neck Surgery. 2020 Jun;31(2):120-7. https://doi.org/10.1016/j.otot.2020.04.008
Lipp M, Golecki N, Merz U. Fiberoptic Intubation: An Introduction and Review of Case Histories: Endo-Press; 2014.
Ahmad I, El-Boghdadly K, Bhagrath R, et al. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia. 2020 Apr;75(4):509-28. https://doi.org/10.1111/anae.14904
Puchner W, Egger P, Pühringer F, Löckinger A, Obwegeser J, Gombotz H. Evaluation of remifentanil as single drug for awake fiberoptic intubation. Acta Anaesthesiol Scand. 2002 Apr;46(4):350-4. https://doi.org/10.1034/j.1399-6576.2002.460403.x
Santonocito C, Noto A, Crimi C, Sanfilippo F. Remifentanil-induced postoperative hyperalgesia: current perspectives on mechanisms and therapeutic strategies. Local Reg Anesth. 2018 Apr 9;11:15-23. https://doi.org/10.2147/lra.S143618
Sanfilippo F, Conticello C, Santonocito C, et al. Remifentanil and worse patient- reported outcomes regarding postoperative pain management after thyroidectomy. J Clin Anesth. 2016 Jun;31:27-33. https://doi.org/10.1016/j.jclinane.2015.12.025